As the retirement boom approaches, biomeds eye thinner ranks and the encroachment of IT

Average base salaries of senior BMET 3 by region. (Click to enlarge)
In some respects, little has changed across the healthcare technology management (HTM) landscape since this time last year. 24×7’s 2015 survey of job satisfaction and compensation revealed that despite ongoing stresses and uncertainties—and wide acknowledgement of the growing role information technology (IT) will play in the profession going forward—biomeds remain largely positive about their careers and compensation.
Ninety-three percent of respondents indicated they would recommend the HTM profession, and many praised the job’s flexibility, variety, and potential to help others. “It’s like Christmas every day!” enthused one participant. “You never know what each day has in store for you.” Said another, “I enjoy helping staff help their patients,” while a third cited “the reward of knowing that I took something broken and brought it back to life.”
But signs of a sea change are unmistakable. For the first time, this year’s survey queried respondents about their timeline for retirement in an effort to gauge which regions will first feel the effects of the Boomer exodus from the workforce. The data confirmed what many in HTM already know intuitively to be true: Starting in about 5 years, the field will see a major wave of retirement lasting about a decade, although we’re already on the edge of the upswing.
Needless to say, this trend poses a major challenge to the profession. Those remaining will have to solve tough problems, including developing strategies to recruit, train, and retain talented young people, defining the role HTM will play in managing networked medical equipment, and determining best practices to defend against cyber attacks.
And though conflicts with IT remained top of mind for the majority of respondents, this year a growing awareness of the demographic shifts in play was also evident. “A lot of us are in the over-40 crowd. When younger people do work in our field, they almost always find something [else] that pays better or attracts them more,” commented one respondent. Lamented another: “Too many old folks retiring and not enough new blood.”
Methodology
[sidebar float=”right”]
States by Region
New England
CT, MA, ME, NH, RI, VT
Middle Atlantic
NJ, NY, PA
East North Central
IL, IN, MI, OH, WI
West North Central
IA, KS, MN, MO, NE, ND, SD
South Atlantic
DC, DE, FL, GA, MD, NC, PR/VI, SC, VA, WV
East South Central
AL, KY, MS, TN
West South Central
AR, LA, OK, TX
Mountain West
AZ, CO, ID, MT, NM, NV, UT, WY
Pacific
AK, CA, HI, OR, WA
[/sidebar]
This year’s survey was conducted by Readex Research, a Minnesota-based research firm, on behalf of 24×7. The study was graciously sponsored by GE Healthcare. Invitations to complete the 33-question online survey were e-mailed to 24×7 subscribers on September 9, 2015, with reminders sent on September 14 and 17. The questionnaire included inquiries about respondents’ education, salary, benefits, job satisfaction, and workload, as well as their opinions on the key issues facing the profession.
Of the 1,322 subscribers who participated, 1,183 indicated they were employed full-time as an HTM professional in the United States. Results from the first 1,100 respondents were tabulated for analysis in this report. The margin of error is ±2.8 percentage points at the 95% confidence level.
The salaries noted here are based on median values, as opposed to averages, in order to prevent skewing the data with extremes. Like last year, we’ve broken out salaries by nine geographic regions to reflect the high response rate. However, due to smaller sample sizes for certain job titles, such as clinical engineers, some categories did not include enough responses to generate a reliable median. Those instances are marked with “N/A.”
A Picture of Stasis
The absence of young recruits across the workforce was mirrored in the survey results. This year’s “typical” participant is a 52-year-old senior BMET working at a 300-bed hospital employing a team of eight biomeds. He lives in the South or Midwest, perhaps in Ohio or Texas. A certified CBET with an associate’s degree, he has accumulated 22 years of experience and served his current employer about 13 years. Although he averages 44 hours per week, he’s not currently searching for another job or pursuing another degree. He’s mostly happy with his compensation and benefits. He plans to retire in about 13 years.
As has been the case in previous years, the largest proportion of 2015 respondents—exactly one third—indicated they were employed as senior BMETs; those identifying as BMETs 1, 2, or 3 made up nearly half of all respondents, at 48%. Managers formed the next highest proportion, at 17%, followed by imaging specialists at 14%. Directors and executives accounted for 9%, clinical engineers for 3%, and 8% of respondents marked “other.” One percent did not respond. The vast majority of respondents—81%—work in a hospital, medical center, or multihospital system; of these, nearly a third (31%) work in mid-sized facilities with 200 to 399 beds.
The age of respondents was consistent with previous reports on the graying of the profession: The median age was 52, with 57% indicating they were 50 or above. The proportion of women in the field also stayed more or less steady when compared with data from the last 2 years, at 8%. In terms of geography, not all areas were represented equally: Two thirds of respondents reside in the Midwest or South (at 32% each), with smaller pools of respondents coming from the West and Northeast, at 20% and 15%, respectively.
Modest Gains
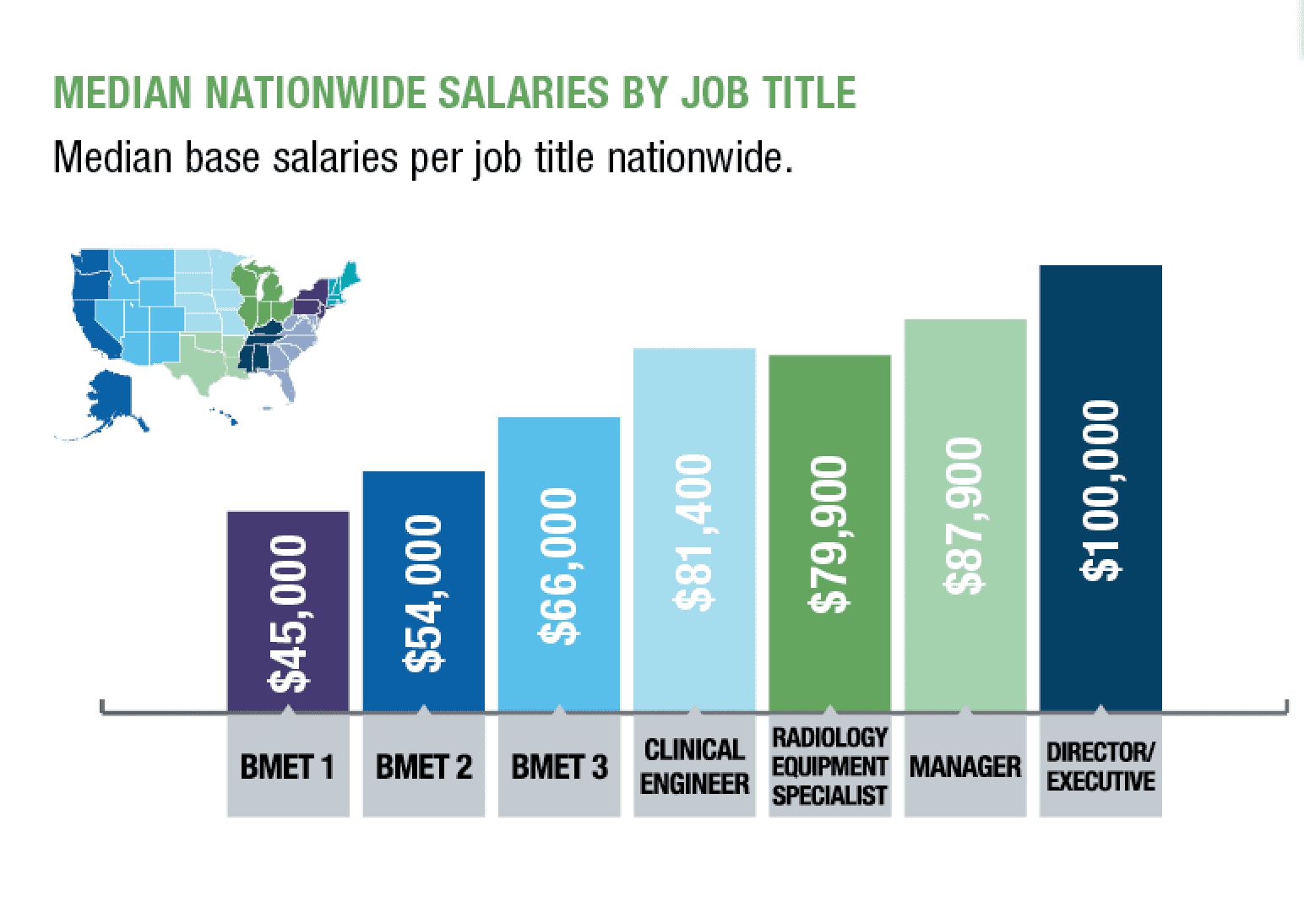
Median base salaries by job title nationwide. (Click to enlarge.)
Overall, HTM professionals saw their salaries rise this year. Senior BMETs’ pay held fairly steady, with a raise of slightly more than 2% and a nationwide median of $66,000. But wage increases compared to last year’s data ranged from more than 4.5% for entry-level BMETs ($45,000) to 5% for imaging specialists ($79,900), 6% for clinical engineers ($81,400), 8% for mid-level BMETs ($54,000), and almost 10% among managers ($87,900). Directors and executives were a notable exception; their salaries dropped more than 9% from 2014, to $100,000.
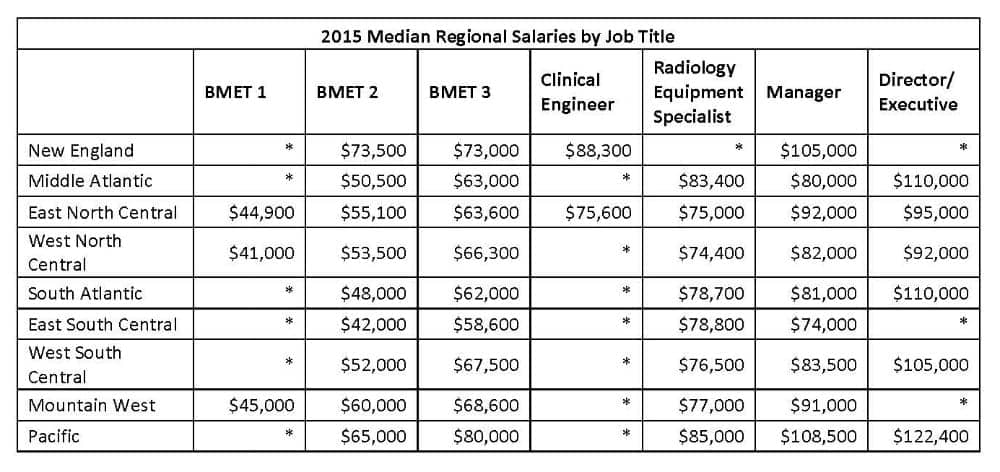
Median base salaries for HTM job titles by region. (Click to enlarge)
Pay also depends on the type and size of the employer. In a shift from last year, hospital-based employees fared slightly worse than their counterparts at independent service organizations: At $70,000, the former earned $2,000 less than employees at ISOs. Both groups, however, were out-earned by employees of medical device manufacturers, who take home a median annual salary of $88,000. Among those working in medical facilities, annual pay increased along with HTM headcount: Biomeds at hospitals with fewer than five department employees saw a median annual salary of $65,000, while those in departments with 15 or more members earned $80,000.
HTM professionals continue to enjoy generous benefits, with 99% of respondents receiving health insurance, and only slightly lower numbers reporting dental, vision, and life insurance. Despite belt-tightening at many hospitals, just over half (51%) of respondents still receive a budget for professional development opportunities like attending conferences. And 73% earn tuition reimbursement—particularly valuable given the strong correlation between education and pay, as we’ll see below.
A Certifiable Difference
When it comes to education, it pays to go to college. Annual wages increased markedly with each additional degree—about $12,000 per diploma—although this year, as in past surveys, only about a fifth of respondents indicated they are currently pursuing further formal education. On a scale of 1 (very unsatisfied) to 5 (very satisfied), those with an associate’s degree reported the lowest satisfaction with their compensation, at a mean rating of 3.6, compared to 3.9 for respondents with military training and 3.8 for those with a BS, MS, MBA, or PhD.
And although one respondent grumbled, “Right now no one cares about certifications, they will give you a small raise and that’s it,” 55% of respondents report having at least one credential—but which one appears to matter a great deal to income. The certified biomedical equipment technician (CBET), the most popular by far at 40% of the survey population, led to a bump of only about $5,000, or 8%. That’s significant, however, considering this raise accounts for almost half the jump a biomed could expect from acquiring another formal degree. The certified radiology equipment specialist (CRES) was nearly three times more profitable, linked to a median salary 21% higher than those with no certifications.
In what will come as little surprise to biomeds annoyed by disparities between HTM and IT pay scales, the most bang for your educational buck exists across various IT certifications. Although (or perhaps because) they are found in such a small portion of the survey population, they remain fairly lucrative. Those with an entry-level A+ certification reported annual median wages 9% higher than the uncertified baseline; for professionals with the mid-level Network+ certification, that margin doubled to 18%. And for the 2% of the survey population with a certified computer examiner (CCE) certification, median salary skyrocketed to 56% above the uncertified median.
Where Are the Women?
Women made up only 8% of this year’s respondents. The largest proportion, like their male counterparts, are mid-level or senior BMETs. Only 4% of this year’s respondents listed themselves as entry-level BMETs, which could reflect the tapering off of younger entrants to the field in general. Twenty-two percent are managers or directors.

Female HTM professionals by job title. (Click to enlarge)
Of particular interest was how female HTM professionals stack up against their male counterparts in terms of distribution by job title. Relative to their representation in the population, women are more likely to be junior or mid-level BMETs. (They also made up only 4% of the survey population with 30 or more years of experience, suggesting that on average the women surveyed joined the field later than men.) Women were least represented among the imaging specialist population: The survey counted only one.
Despite these distinctions, women appear nearly as likely as men to hold positions of authority at the manager and director level, comprising 7% of those populations. And while respondents reported a gender wage gap of $11,000 at the manager level (a shortfall for women of 12.5%), female directors slightly out-earned their male counterparts by 4%.
Not for Everyone
On the whole, HTM professionals are content with their pay: On a scale of 1 (very unsatisfied) to 5 (very satisfied), 64% of respondents rated their salaries a 4 or 5. The majority also indicated they felt very or somewhat fairly compensated according to their experience (54%) and education (59%).

Median salary by percentage of respondents and satisfaction level. (Click to enlarge)
Among the vast majority of survey participants who said they would recommend the HTM field to others, many detailed the rewards of working in healthcare. As noted earlier, respondents endorsed HTM as “worthwhile work with a purpose” and “an honorable profession,” while one praised “the ability to meet and interact with different people.”
But tellingly, even middling responses noted the profession’s growing number of drawbacks. “It’s not for everyone,” several respondents acknowledged. “Not as fun as it used to be,” said another. Further down the scale, those who rated themselves least likely to recommend HTM cited lack of recognition or opportunity and pay unequal to the job’s aggravations. One respondent called HTM a “dead-end career,” while another wrote, “Career development consists of going to an OEM school and that’s it.” A third concluded, “This is a thankless profession.”
A Heavy Load
As in previous years, biomeds continued to share tales of tremendous workloads: This year, more than two thirds categorized their responsibilities as heavy or excessive. When asked to elaborate on their ratings, respondents were eloquent in sharing accounts of understaffed, overworked departments scrambling to fill gaps across their healthcare system.
“We have four full-time positions posted that my organization cannot fill,” one respondent wrote. “It is well known in my area that my employer does not compensate, and we do not get qualified applicants. Instead of hiring and training, we do not hire, and the jobs stay open. We are 2 months behind on PMs and have taken over much of the server environment, without adding staff.”
“We had a consultant come in and say that we are about nine people short for the amount of equipment we have in our facility. That was about 2 years ago,” said another. “Since then, we have expanded and have plans to lease several other buildings in 2016.”
“Over 9,000 medical devices to service,” wrote a third. “Workload can be unbearable if a BMET takes a day off.”
Go West, Young Man
Soon, those workloads may get heavier. More than a third of HTM professionals plan to retire within the next 9 years. Stretch the forecast to 15 years out, and more than half of workers—55%—expect to depart.
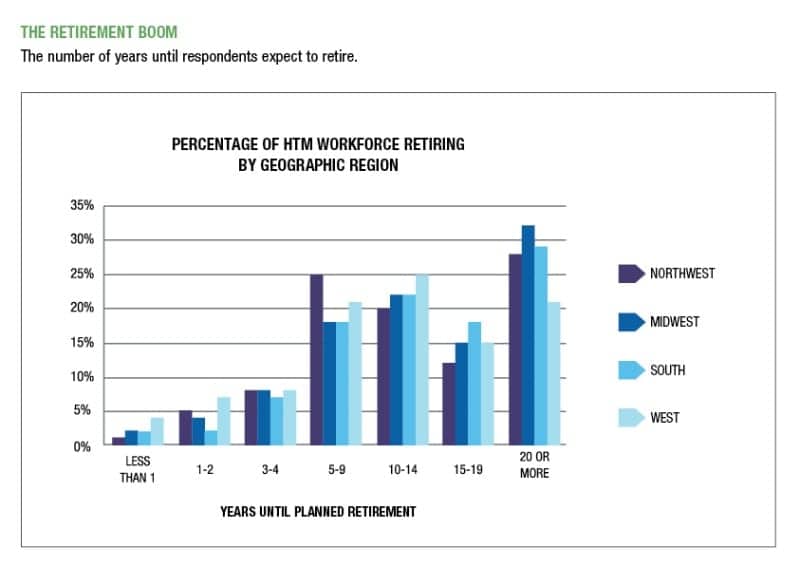
The percentage of the HTM workforce retiring by geographic region. (Click to enlarge)
For younger biomeds willing to relocate, the coasts may offer the best, and earliest, opportunities for advancement. The West barely edges out other regions with the oldest workforce, at a mean of 51.4 years old, but 11% of workers there plan to retire within the next 2 years. The trend then slows a bit, as 19% of workers in the West plan to end their careers over the next 4 years.
Following the West, the Northeast will see a significant spike 5 to 9 years out, as 25% of its workforce retires, but the rest of the country won’t be far behind. During that same period, nearly one fifth of HTM professionals across the United States will retire. In contrast, almost half (47% each) of the population in the South and Midwest currently plans to work 15 years or more. Those regions also have a slightly younger average age, at 49.9 in the South and 49.4 in the Midwest.
Turf Wars with IT
While the retirement boom may well prove the profession’s most serious long-term obstacle, immediate concerns were largely focused on the fraught relationship between HTM and IT. Conflicts between the two departments ranked as the single highest burden for many respondents. Other frequent complaints included lack of respect, clueless management, uncooperative OEMs, inadequate training, cost cutting, and the challenge of keeping up with constantly evolving regulations and technology.
“Biomeds will continue to do more work than IT personnel and receive less compensation and prestige,” predicted one respondent. While the two departments have come a long way, another noted, “much work is needed to tear [down] the walls between ‘us’ and ‘them,’ ‘yours’ and ‘mine’ to make both sides feel more empowered in maximizing patient care.”
In the near future, the field may discover that solutions to its key problems are linked. As older biomeds retire, the profession will have to welcome (or find) younger replacements. These entrants may see a less extreme divide between HTM and IT than their predecessors did. They may also be likelier to have—or at least willing to acquire—the technical know-how so urgently needed. Until then, those who want to ride out the next decade will have to learn to adapt.
Or in the words of one respondent: “The advance of ‘smarter’ medical equipment means that now, more than ever, it is important to gain skills beyond simple PM and calibrations.”
Jenny Lower is chief editor of 24×7 magazine. Contact her at [email protected].



Many hospitals are now combining HTM and IT departments. For the radiology engineers I thought the salaries were a little low, but then again I suppose it is based on how many different modalities you are competent in servicing. Thanks for the article!
What a wonderful survey! Some of the results are to be expected, like the higher salaries out west. But there are some surprises, too. For me, I am surprised that Radiology Specialists aren’t earning more, and that more folks aren’t pursuing certification or additional education.
If I were managing people, I would be concerned about the numbers of retirees in the next few years. Even if they weren’t my own staff, there would be a lot of openings that could lure my staff to other positions. Keeping your good staff happy and engaged and loyal has never been more important.
Good work, 24×7 and Jenny.
I am one of those 50+ senior CBETs. For me I see too many youngsters coming up that got degrees and a lot of education. But they have little practical skill with hands tools and 4 dimensional critical thinking. The educators in biomed programs should have complex pieces of equipment and students should be drilled in tear down and rebuild. They need to be taught what medical equipment really is on the inside. Also learning to work with caregivers is a skill that needs to be taught. We fix people with technology issues. Millennials seem to me (in general) to be ill-equipped to fix a complex system that includes caregivers, patients, a hospital, and technology in a complex matrix. As for the IT professionals, we will always be ahead of them in the care environment as they are not creatures that can live in the same atmosphere as we biomeds do. What are your thoughts about my post here?
Scott, I am one of those educators who strives to teach students the skills they need to be excellent technicians and effective members of the clinical team. We partner with local hospitals to expose students to a wide variety of devices. However, as long as hospitals hire graduates from programs without hands on experiences/internships or schools without equipment, we will not see the amount of high quality technicians the profession needs. Hospitals must demand and partner with schools to ensure high quality training…Oh, and don’t decline to take interns…when hospitals say no (and they do here in Indianapolis all the time), I struggle to find placements for students…
Hospitals and educational institutions need to act as a team to produce technicians!!!
Thanks for a great article, I am one of the rare female techs with nearly 25 years in the field of biomed. I have not pursued certification as there has not been an advantage in doing so. I consider getting further training in the IT field to become more comfortable with the ever advancing technology but do not see a clear path to focus on. How do we know where to aim our IT arrow to maximize skills and usefulness in our own field and prepare for my remaining 15 years? I would love to hear from both Patrick Lynch and Barbara Christe.
Susan, I am happy to comment on certification…first, let’s clarify the type of certification you are considering. CBET certification is specific to our discipline and offers a credential recognized by our profession to document competence. Perhaps you are asking about IT certifications like NET+ Either certification type can be desirable professionally, depending on your employer, or as a tool to document a personal achievement. Your preparation for certification is an opportunity for lifelong learning and personal growth – which may or may not be rewarded by your employer. Determining what is valued in your workplace is a great place to start. Good luck!!
Susan, I am a believer that you can never have too much education, training, or letters behind your name. You never know what opportunity will present itself in the future, so to be prepared for it it the wise thing. I know lots of Biomeds who have moved into IT, Epic and all sorts of IT integration. Let’s face it – we know the patient care technology and are the base equipped to make it work to the needs of the caregivers. Yes – go for any IT certifications.
Thank you for a great article. I am 1% of the female population in the Imaging Field. I have been working in imaging now for 12 years, and I am also CRES certified. I hope those in our field (Imaging or Biomed) look at advancing their careers with degrees or certifications, not solely for pay, but to push and develop themselves more. We work in a field of rapid growth, you have to evolve with that growth if you want to see a change in pay, position, or influence. This is a rewarding line of work with numerous possibilities for those who wish to take them.
I’m one of those future retirees and have been a BioMed Manager for 35+ years. What I have found that has worked for me is to hire people that have Ambition to learn, a positive Attitude about their work and life, and some Ability in electronics/mechanics with practical thinking skills. Using this concept in hiring has always been successful for me and my customers. I’ve had and have today some excellent technicians many who have moved on to run their own departments at other hospitals. It is not necessarily always about the education or the letters after one’s name but it is more about the person. I think our field is a excellent career choice for someone who wants to make a difference and it’s not always about the money, which I believe is very good in this profession.
Hello Wayne R. Jenkins, Am a recent graduate of Vincennes University as a Biomedical Equipment Technician. What is your best advice for recent graduate like me that is about start a life long career in this field?
Being in this industry since 1975 and having the opportunity of holding positions within in-house, ISO and OEM organizations ranging from field service engineer to VP of Operations, I find that there are still a lot of questions that people may not understand. OEM personnel are going to earn more than in house and looking at the service rates you are charged for their service will explain a good portion of that. ISOs earn more than in-house because those companies are buying your knowledge and education of certain products and service capabilities to fill a need that they have for a contracted customer. In-house personnel are sharing the responsibility of the operational costs of health care today and unless you have an administration that recognizes your value as a “cost savings” department and that you show the return on investment of your personnel, you are going to experience as frustrating future. Our technology has been changing and the advantages that an in-house technician has is receiving the OEM training and has familiarity with the environment. I have for the last 10+ years have stated that a BMET should have a strong familiarity with IT, almost to the point of being called a BMIT, since almost 50 cents on every dollar being spent today in hospitals is IT related to the electronic health record, the networks and security. IT doesn’t want to touch the patient care equipment so this is to your advantage.
It’s important to understand that if you are looking to succeed in this field is that you must want to succeed, want to work to succeed, learn as much as you can and go to where the opportunity can take you.
Hi Lary Sheppard, I was reading this article today and I came across your comment on this article. MY question is, As an Experienced CBET professional for over 30+yrs of experience, what is your best advice for a young student like me that just graduated with an Associates Degree in Biomedical Equipment Technology, and what are the best routes to take later in this field of Biomedical Technology in terms Money and work life balance?
Hello my name is Thu Nguyen and I was wondering about where do radiologist equipment specialist usually work at. Do they only work for manufacturing companies and ISO or do hospitals usually have a separate department for them.
Also what are the working hours like.
What are your advice for someone who just graduated in this Biomedical field, and what are the best routes to take after getting an Associate degree in Biomedical Equipment Technology