|
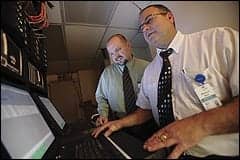
| Mark Wentworth, senior clinical engineering technician, Crouse Hospital, Syracuse, NY. |
No department is an island, not even clinical engineering. They are more like pools—of resources. And, as technology advances, those pools become deeper and wider. Russell Taylor, senior clinical engineering technician, just celebrated his 31st anniversary at Crouse Hospital, a 575-bed facility in Syracuse, NY, and has witnessed this change firsthand.
“When I first started, we were two technicians, a box of parts, and a notepad for inventory,” Taylor says. “Now, we have inventory control and computers with the assets and equipment database and histories.” At Crouse, the clinical engineering department has drawn on its expanding pool of resources to “make a splash” in patient safety, employee and customer satisfaction, and cost savings—$800,000 since July 2008.
Much of this money has been realized through reductions in capital investments. The participation of clinical engineering in the acquisition process has enabled the facility to extend the life of existing equipment that it would likely have chosen to retire without the clinical engineering department’s input. A clinical engineering management contract with ARAMARK Healthcare, based in Philadelphia, has provided buying power and innovative resources so that Crouse benefits from volume purchasing and the ability to find discontinued parts when making capital equipment decisions. In addition, biomed rounds permit clinical engineering to draw on the facility’s internal resources, allowing users to help identify problems and opportunities, and prevent small issues from turning into larger ones.
The interaction of Crouse’s clinical engineering team with the medical community at large is equally valuable and mimics the internal interdependency that has been critical to its success. Crouse’s biomeds participate in the FDA’s device safety initiatives: the Medical Product Safety Network (MedSun) and its pediatric offshoot KidNet. Not only does the Crouse team report device problems and concerns within the FDA network, but it also uses the FDA databases and other resources to expand its own equipment research and service capabilities. “It’s not just something we touch upon once in a while. It’s part of our day to day,” says Christopher Murphy, clinical engineering manager at Crouse Hospital for ARAMARK Healthcare.
The team’s day-to-day efforts differ with each earthly revolution but are tackled with whatever resources are available, from technology to staff to education to innovation.
Capital Contribution
The Crouse clinical engineering department oversees 6,600 devices with a team of six clinical engineers, two imaging engineers, and an administrative assistant. Together, they handle most of the medical equipment in-house, including radiology (or at least portions of radiology service) and the clinical laboratories. The team’s vast knowledge of the wide variety of equipment is due in part to experience—many of Crouse’s biomeds have 20-plus years on the job—and in part to education, through acquisition contracts, ARAMARK Healthcare training opportunities, associations, and regulatory agencies, such as the FDA.
 |
| L-R, the Crouse team: Claire Rouse, administrative support; Russell Taylor; Adam Gaal; Christopher Murphy, clinical engineering manager; Rick Buza; Chris Langmeyer, CBET; and seated, Mark Wentworth. |
This knowledge is also key in evaluating equipment for capital purchase decisions. A new policy requires clinical engineering’s participation on the hospital’s capital request committee and approval of all requests, giving biomeds the opportunity to find more cost-efficient solutions, should they exist. And they do—in more than one instance the clinical engineering team has been able to save the hospital money through the refurbishment of existing equipment.
Prior to going to the capital request committee, many departments will go to clinical engineering first, where Murphy and the team review the request and decide the best match for the hospital, the end user, and the patient. Although each piece of equipment is evaluated individually, the team does have a few guidelines.
“We look at what kind of parts are available and how long they will be available for,” says Chris Langmeyer, CBET, clinical engineering supervisor.
For example, the team was asked to review a request to purchase a new surgical microscope. The evaluation of a scope in storage, however, revealed it could work instead.
“The scope had a solid base, solid arm, and no rust,” Taylor says. “It looked like a good unit. We’ve had other microscopes in the past that you just look at and see no reason to even pursue.”
The old microscope could be brought up to the standards the clinicians required, and so the determination was made to update the instrument. With an infusion of $5,000, the team was able to refurbish the microscope, put it back into service, and save the hospital $45,000.
Of course, not every piece of equipment can be saved, but when new purchases are made, the team still aims for cost efficiency and will standardize devices where possible. Clinical engineering is currently working to match vital signs monitoring throughout the hospital. Wall-mounted patient monitoring units have already been standardized throughout the operating rooms, intensive care units, emergency department, labor and delivery, and the neonatal unit.
This means regardless of where a clinician or biomed is in the hospital, monitoring devices are the same type of equipment.
“Not only does that provide better continuity of care for the patient, but it’s easier training for the nurses,” Langmeyer says. “Conceivably, a nurse could go from the neonatal unit to the OR and, from a monitoring standpoint, have [to undergo] little to no training.”
Standardization also makes the biomed’s job easier. “We have just one or two service manuals and a selection of parts that are interchangeable with any of the monitors,” Taylor says. The department therefore saves storage space and time; with a ready supply of parts and exchangeable equipment, turnaround time is decreased, uptime increased.
Purchasing Power
Whether a decision is made to refurbish or replace, additional savings can be realized through the organization’s association with ARAMARK Healthcare. “Opportunities are pretty commonplace since we’ve been put on the capital request committee, where we are able to get between the buyer in the clinical department and the buyer in the purchasing department and see what ARAMARK Healthcare can do with their purchasing power and economies of scale,” Murphy says. In addition to obtaining volume discounts, the organization may also have better resources in locating discontinued parts and the expertise needed to use them.
For example, ARAMARK was able to find the same optical binoculars, a microscope accessory, for $7,000 versus the hospital’s $10,000 pricing. A $350,000 estimated new replacement radiology room cost only $10,000 when refurbished with Crouse engineering knowledge and ARAMARK purchasing power. “They were able to find parts that were needed but no longer in production,” Murphy says.
Similarly, Crouse turned to the ARAMARK purchasing network to find a backup control board for a cart washer that would cost $200,000 to replace new.
“Cart washers use basic plumbing components that you might be able to pick up at a Home Depot or Lowe’s,” Murphy says. “The one Achilles heel to this unit was a control board no longer in production, but, through ARAMARK Healthcare, I was able to find it, purchase it, and put it in stock in case the board does fail.” The hospital was able to apply the budgeted $200,000 elsewhere.
Although Murphy has been on board at Crouse for only the past year, the hospital has partnered with ARAMARK Healthcare for 6 years. Murphy is employed by ARAMARK, but Crouse employs the rest of the clinical engineering team.
“The relationship is a very large resource for information for us that we might not have had access to had we been strictly managed by an in-house manager,” says Mark Wentworth, a Crouse senior clinical engineering technician.
Running Rounds
Another excellent source of information has developed through the internal rounds the biomed team makes every morning throughout the facility. “All of us, as technicians, have assigned areas in the hospital, and the first place we go to after getting to work every morning is the rounding area,” Langmeyer says. With the exception of the imaging technicians, duties were assigned fairly randomly, reflecting the depth of knowledge among the team members.
Langmeyer is responsible for visiting the neonatal and perinatal areas, checking in with the nurses to make sure no problems developed with the equipment overnight. “It’s increased their communication with us so that they bring issues to us a lot earlier, which allows us them to solve them a lot quicker,” Langmeyer says.
Murphy performs quarterly roundings with directors and managers, taking however much or however little time they have to give. “It’s really getting in front of them and letting them know constantly that we are there,” Murphy says.
The reminders work—Murphy notes that request lists grow, rather than shrink, every time he holds another meeting with a department head. “They recognize their part in our department’s success and prepare a list for ideas and needs,” he says.
The techs appreciate the ability to communicate daily with clinicians, finding it makes the job both more pleasant and less challenging. “I think communication with the customer base is key and that a program, like the rounding program, that keeps the communication open with your customers is the best route to success and job satisfaction,” Wentworth says.
Constant Communication
Once the comfort level is established, communication extends outside of rounds to other methods and does not always have to be face-to-face. “We’re comfortable as a team, they see us every day, and they know us,” Taylor says.
 |
| L-R: Chris Langmeyer, CBET, and Rick Buza—part of Crouse’s clinical engineering department that oversees 6,600 devices. |
The Crouse clinical engineering department can be reached via phone and the Internet. “We don’t depend just on one method of communication,” Wentworth says. “We try to keep open as many avenues of communication as possible to get that information from the customer to us and vice versa: telephone, e-mail, the database, the rounding-out program.”
Outgoing information can be as useful as incoming. Communicating before and after preventive maintenance efforts typically enlists the clinical department’s help in locating and accessing the equipment needed for service. “E-mail can be dangerous sometimes because you’re doing all the communication behind a screen, but if you use it for quick, simple messages to keep people in the loop, everyone is happy,” Murphy says.
Within the clinical engineering department, the administrative assistant keeps track of incoming service orders, whether arriving in an e-mail, through the online database, or by phone. All orders are placed on a physical service board and in the database, which includes all the information regarding the inventory and device service, such as purchase orders, manuals, and service reports. Crouse’s clinical engineering department is completely paperless, and whatever is not already electronic is scanned and captured digitally.
The technicians carry PDAs that sync their data to the database at the end of each workday. Mobile biomeds can print asset numbers, open work orders, and monitor worklists in the field, “while they’re waiting for the elevator, while they’re walking down the hallway, while they’re waiting for a device,” Murphy says.
Cell phones, a shared on-call pager, and the Intranet increase the biomeds’ accessibility, making some information immediately available to clients. Appropriate employees can use the hospital Intranet to access a searchable clinical engineering application with information on devices and work orders.
“If someone is wondering what’s going on in a radiology room, they can enter that asset number and learn up-to-date, real-time information: ‘we are waiting for a part’ or ‘the unit is being tested,’ ” Murphy says. Users can obtain the immediate information they need, reducing the administrative time on both sides. “They can get the information that’s pertinent to them, and we’re not bombarding people with information they are not really interested in or that they don’t need to know about,” Murphy says.
In-house surveys show that customer satisfaction has improved by all benchmarks over the past year, and though communication ratings also went up, there is still room for growth, according to Murphy. “We usually do rank lowest in communication—albeit it’s still a 4.5 [of 5.0]—but we need to work on it,” he says.
Bigger Pools
Murphy also admits the hospital’s participation in the FDA’s MedSun and KidNet programs has room for growth, though it too has shown significant improvement since its launch at Crouse in February. “We have 2,600 people in this hospital, but slowly, we are getting there, and it’s almost on a day-to-day basis where someone from clinical engineering is coming to me with an idea or an opportunity they recognize for product improvement and that they feel the FDA should be involved in,” Murphy says.
MedSun is an adverse event reporting program of the FDA designed to identify and solve medical device problems before serious injuries and/or deaths occur. The offshoot, KidNet, focuses on devices used in neonatal and pediatric intensive care units.
Reporting facilities, which number about 350, are asked to provide information on adverse events and “close calls” though an online database with restricted access. Murphy notes he completed a 2-hour tutorial before being approved to use the system. Even so, the real challenge has been to increase awareness and reporting throughout the hospital’s departments; the effort has been embraced by the biomed team.
“When the staff is out making the repairs and interacting with end users, they are always cognitive of the fact that what they are dealing with or what they are hearing might be something that should be reported to MedSun. That’s something that we’re trying to influence the end users to do as well,” Murphy says.
The extra work is rewarded with extra resources. The team has access to the FDA and its searchable databases, which Murphy refers to as a massive collection of information about medical devices as well as end user experiences. The information can be mined to assist with acquisition decisions as well as maintenance and repair efforts.
“It’s a big sharing resource, where we can find out if other people are having the same issues and see what their resolutions might have been,” Langmeyer says.
Inner Resources
Of course, the first resource drawn on when a problem arises is the knowledge within Crouse’s clinical engineering team. “Some of the team members have been here for 30 years, and with that much time on the job, they are an absolute encyclopedia of knowledge,” Murphy says.
To make sure that knowledge grows, the hospital encourages continued education, both formal and informal. The partnership with ARAMARK Healthcare has provided training opportunities to the team through the company’s Technical Resource Center in Charlotte, NC. For instance, Crouse employees have been trained through ARAMARK on sterilization techniques, including the use of steam and peracetic acid.
On-the-job training is also invaluable. Murphy prefers that staff attempt to repair a device rather than rely on another expert. “If you bring the manufacturer in to make the repair for you every time you are unfamiliar with a problem, no one is learning anything,” Murphy says. Trial and error is considered more valuable to the team than an unsuccessful repair attempt. “You learn so much more from it,” Murphy says.
|
Read past department profiles in the archives. |
And the team is not stingy with its knowledge. In addition to MedSun/KidNet participation, Crouse is also working with a locally based international medical device manufacturer to aid its research and development team. The agreement is in the preliminary stages with details remaining to be worked out, but Crouse has provided its patient population to the manufacturer for some of its statistical studies.
The opportunity to contribute to the development of potentially life-saving medical devices adds to the satisfaction of the Crouse clinical engineering team, who are always up for another challenge. Their consistent performance has, thus far, awarded them the freedom to tackle new challenges for the benefit of the department and the hospital, and permitted them to dive into whatever resource pool they need.
Renee Diiulio is a contributing writer for 24×7. For more information, contact .