
The 2018 American College of Clinical Engineering (ACCE) Body of Knowledge (BOK) has unveiled the results of their 2018 survey of HTM professionals. The 2018 BOK Survey was created for a unique purpose: to determine the current scope of practice and knowledge base for clinical engineers (CEs)—information the U.S. Board of Examiners will use to design the clinical engineering certification (CCE) exam. By doing so, the exam board can better match the test content to the needs of clinical engineers.
2018’s survey was updated from the 2015 version to include CCE exam eligibility, new certifications, and additional knowledge topics. Compared to previous years, the survey was also open for a longer period, lasting through the annual conferences of both the Healthcare Information and Management Systems Society and AAMI—for a total of roughly six months. Due to various factors, including the longer survey window, survey participation increased 13% from 2015.
Fortunately, the survey results were very telling, with the data collected providing valuable insights into the CE profession. In addition, the analysis of the data presented in this article allows for several significant conclusions about both the data itself and the survey process as a whole.
Survey Demographics
U.S.-based professionals accounted for the vast majority of respondents (67.2%), with Brazilians trailing Americans as the second-highest represented nationality at 9.7%. Most participants work in a hospital, clinic, or health system (68.2%), and a majority identify themselves in healthcare technology management positions, an increase from 37.8% in 2015 to 67% in 2018.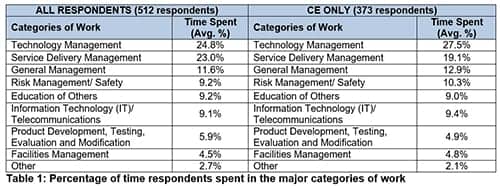
There was also an increase in the number of respondents identifying their current employer as an independent service organization, up from 8% in 2015 to 15%. Moreover, most respondents held either a CCE or CBET certification, with CBETs having the highest percentage at 25%, followed by CCEs (HTCC certified) at 21%. It is notable to mention that many respondents also have the following certifications: IT/networking (23%) (to include CompTIA A+, N+, S+); professional engineering, or PE, (17%); and Lean Six Sigma (16%).
Further, the majority of respondents said they were eligible for the CCE exam (60.5%) and have an engineering degree (76.7%). Additionally, out of the 196 respondents who acknowledged that they were not eligible to take the CCE exam, more than half of them are currently in a CE position. This could indicate that there are more individuals starting their careers as clinical engineers who will become eligible for CCE examination in the near future. This also confirms the interest of the field in the CCE exam.
In the study, respondents were categorized into two sets: CE-only (clinical engineers) and non-CE. The CE-only responses were comprised of individuals who identified themselves as clinical engineers, healthcare technology managers, or clinical systems engineers. The non-CE responses included individuals who classified themselves as biomedical equipment technicians, medical equipment planners, or specialists (network medical systems, radiology, laboratory). Of the 534 responses, 373 responses fell into the CE-only category.
The filtering of data to highlight respondents that identified themselves as CE-only allowed us to better understand the demographics, knowledge, and responsibilities of this group. It also allowed us to make valuable comparisons to the group as a whole (all respondents group) and the non-clinical engineering (non-CE) group.
Technology management and service delivery management were the top two categories of work among all groups, but the order differed depending on the group. Specifically, the CE-only group, which is comprised mainly of engineers and managers, showed technology management as the most important, whereas the non-CE group—comprised mainly of technicians—showed service delivery management as the most important.
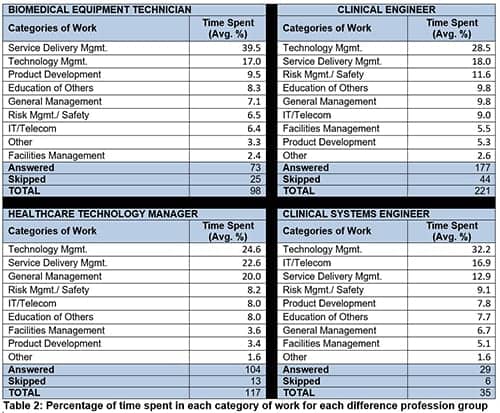
When the work category responses were filtered by position (i.e., biomedical equipment technician, clinical engineer, clinical systems engineer, and healthcare technology manager), IT management was the second-highest work category for clinical systems engineers. This result speaks to the importance of IT integration in their daily tasks.
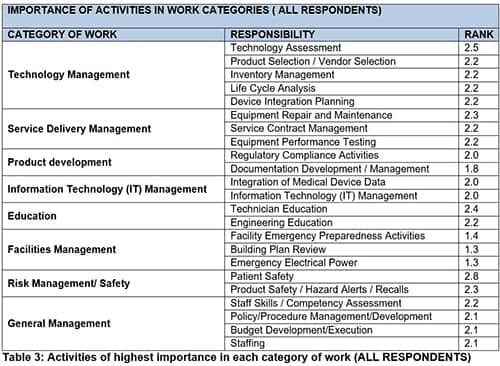
Moreover, the top 10 knowledge categories were the same—albeit with slightly different rankings—between all respondents and the CE-only group. Project management was one of the knowledge categories that was added to the survey in 2018; it was in the top 10 for the all-respondents group and was the second highest in the CE-only group. And of the work categories, survey respondents ranked patient safety as their top responsibility—thus confirming that patient safety is paramount in HTM.
To sum it up, the survey collected a substantial amount of data and provided valuable, current information about the scope of practice and knowledge in the healthcare technology management community and, specifically, in the clinical engineering profession. The U.S. Board of Examiners for Clinical Engineering Certification will examine the survey results and, if needed, update the scope of the exam to better match the attributes of the clinical engineering profession today.
For a more in-depth look at all the data and additional analysis, visit ACCE’s website and view the full 2018 Body of Knowledge survey report.
Katherine Navarro, CCE; Sarah Brockway, MS; Bhaskar Iduri, MS, CCE, CHTM; Renee Huval, MS; Rehman Syed, MS, CBET, CCE; are committee members of the ACCE Body of Knowledge. Questions and comments can be directed to 24×7 Magazine chief editor Keri Forsythe-Stephens at [email protected].


