Clinical engineering departments routinely fall under the IT umbrella these days, but it rarely ends up the other way around. The arrangement often comes down to two factors: money and manpower. “Power in hospitals often rests with those who control the dollars,” says Ken Olbrish, enterprise imaging system administrator, information services (IS), Main Line Health System, suburban Philadelphia. “IT departments are getting more and more money. Clinical engineering departments are not.”
Today, given that nearly all medical devices are essentially networked computers at some level, workflow chart adjustments make sense on many levels beyond pure financial considerations. In 2001, Olbrish had so many overlapping duties within the clinical engineering department that it was not long before he moved to IT permanently to serve in a combination role.
Sporting the “enterprise imaging system administrator” title, Olbrish represents a flourishing breed within the biomedical world—the hybrid. Now officially under the IS umbrella, Olbrish uses his extensive experience in imaging and IT to efficiently support today’s converged technologies.
The continued integration of clinical engineering into IT departments spells a change for the clinical/biomedical engineer—a change that has not been clearly defined. The transition could mean taking on a new CE-IT hybrid role, having to report to a chief information officer (CIO) who may have little or no clinical knowledge, or having to rapidly come up to speed on IT knowledge. Whatever the outcome, the driver of these changing roles and relationships comes back to the convergence of technology.
Some hospital IT departments have addressed the technology convergence by choosing to partner with clinical engineering and bringing the two groups together, thus integrating technology support service. Others have chosen to hire their own clinical engineers, instead of merging with an existing clinical engineering service. IT often makes this move to beef up clinical engineering expertise without taking on what some in IT perceive as the more mundane aspects of clinical engineering—such as preventive maintenance and repair services.
According to some in the industry, splitting these functions—picking up the clinical engineering-IT interface skill set without the service and repair component of traditional biomedical departments—leaves a fractured department that may ultimately weaken the clinical engineering role in the hospital. In addition, this policy still leaves the IT and clinical engineering departments separated when it comes to a problem with connected clinical equipment.
According to Stephen L. Grimes, FACCE, FHIMSS, FAIMBE, chief technology officer and director of clinical systems engineering, Linc Health, Holliston, Mass, this approach reflects how some organizations are dealing with the new realities of increasingly complex and integrated systems. “What had been a clear line between medical and information technologies has blurred,” Grimes says. “Clinical engineering and IT are being forced together to provide the most effective support for today’s converged technologies.”
Being “forced together” may sound like a negative, but many clinical engineers have taken the transition in stride, viewing their changing roles as something that has been a long time coming. While IT may appear more powerful on the surface, Olbrish says he still sees a balance of power and responsibility. Others agree.
“I don’t think either clinical engineering or IT is necessarily more influential,” says Steve Merritt, an infrastructure engineer at Baystate Health, Springfield, Mass. “They both have their niches and specialties. We have a great working collaboration, mainly because we report to the same director. There is a lot of give and take. It’s important that the industry as a whole start working together and stop complaining about each other.”
At Baystate Health, clinical engineering falls under IS and both report to one CIO. One chief unites the disparate tribes, so to speak, and solves any territorial disputes. As one of those “immigrants” from clinical engineering who eventually landed in IT, Merritt says the leadership arrangement works well and allows him to specialize in technology assessment and PACS issues. When it came time to replace the fetal surveillance system at the multihospital system, the CIO coordinated with clinical engineering to house equipment on standardized desktops and servers using the hospital network infrastructure—instead of building separate segregated networks.
Merritt is currently looking for a new nurse call system, but like so many systems these days, the task becomes more complicated with networking. “We are not just buying a nurse-call system,” Merritt explains. “Now you have to figure out how it is going to integrate with your alarm management systems, phone systems, and wireless systems. We try to plot that out on a 5-year map, and clinical engineering has a vital role in that process.”
EMRs Driving Change
At most facilities, IT has grown exponentially in the last 2 decades and has become an essential element in not only finance—where it played its first major role—but in most other clinical and operational areas. According to Grimes, IT is nothing less than the “dominant support service” in the industry. “The most clear evidence of this is IT’s regular representation in the C-suite,” Grimes says. “While clinical engineering and IT may both be technically oriented, the two professions come from two very different cultures. Some aspects of clinical engineering—like scheduled maintenance and repairs—are considered mundane or unattractive by IT, and so we’ve seen some IT services try to take on only those aspects of clinical engineering they more closely identify with—such as medical device integration into electronic medical records [EMRs].”
For better or worse, EMR-related projects are bringing new efficiencies, and occasional headaches, to clinical engineering and IT professionals across the country. One such project for fetal heart monitoring went live at Olathe Health Systems in March 2011.
Clinical engineering and IT worked jointly to configure clinical applications and networking. “We cut over from one fetal monitoring system to a new one, which integrated directly into the EMR,” says Dan DeMaria, manager, biomedical engineering, Olathe Health Systems, Olathe, Kan. “We literally flipped a switch and we were on the new Cerner system. It was a year in the planning phase, and all of the key stakeholders were involved in the process that enhanced data management, waveform management, and alarm management. As time goes on, we will bring in vital signs directly into the EMR as well. If it is data that we gather, it is getting into the EMR, and we want to automate that as much as possible.”
From his perch as head of a major independent service organization, Grimes must routinely seek out the rationale for incorporating new elements into the EMR. Despite the federal government’s efforts to impel medical entities toward EMRs by 2015 through incentives and disincentives, Grimes cautions that the nursing staff must still first verify information (such as blood pressure readings) before sending to the EMR.
One of the reasons for getting medical devices and medical technology onto the network in the first place is to populate the medical record with accurate information, which improves care. Diagnostic devices include things such as vital signs monitors, physiologic monitors, laboratory equipment, medical imaging, cardiac, neurology, EEG, EKG, and fetal monitoring. “There are also therapeutic devices such as infusion pumps, and now there is a big drive to use intelligent infusion pumps,” Grimes says. “All of these elements clearly require the involvement of clinical engineering. The push to deploy EMRs incorporating data from integrated medical devices represents a new major area of collaboration between clinical engineers and IT.”
Even the injectors in cath labs are now networked, monitored, and can flow into the medical record. At first glance, it may all seem excessive, but Grimes points out that the patient benefits are real. “If we see that respiration or blood pressure on the patient is being depressed because of a drug that is being administered in an infusion pump, we have the ability to create closed-loop systems so that the monitor can actually slow down the amount of drug being delivered because it is networked,” he says. “We will increasingly see those kinds of closed-loop systems. This is a trend that will only accelerate in the coming years.
“We are building intelligence into the systems and removing some of the need to make those clinical decisions that are more straightforward,” Grimes adds. “To the degree that you can remove some of the variability and potential for human error from the equation, that is a positive thing. These are areas where IT and clinical engineering need to work together to make this all run smoothly.”
Integrating the Healthcare Enterprise (IHE)—an initiative by both health care professionals and industry members to improve the way computer systems in health care share information—has made things easier by encouraging the development of systems that can work well together, even if they are from disparate manufacturers. It started with imaging systems 10 years ago and has now migrated into other medical devices. “If you buy Alaris, Philips, or GE, and they are subscribing to the IHE adopted standards, you know they will work well together,” Grimes says. “And that is going to help with medical records as well.”
A New Way of Thinking
Paradigm shifts in any field may come gradually, while others can be traced back to an exact moment. DeMaria remembers a day in the 1990s when everything changed. The former Army medic was maintaining heart cath labs when DICOM appeared on the landscape. Instead of generating images on 35-mm film, officials asked him to bring digital images onto a network and hard drive to display on computers. “That was the day it occurred to me that this field was about to change,” DeMaria says, a 28-year clinical engineering veteran with 4 years at Olathe. “My personal journey began that day, and I started learning about computers and networking. Of course, we all went kicking and screaming, because change is painful.”
Clinical engineering and IT departments at Olathe are officially combined, and both entities work together to take care of 5,000 pieces of equipment at a 300-bed institution, in addition to a 28-bed facility and 34 clinics. Similar to Baystate Health, all report to a CIO, an arrangement that is now increasingly common.
DeMaria hired on 4 years ago to help facilitate the transition to one unified division under IT, and he admits that full integration took time and patience. “I was invited to weekly IT manager meetings with the CIO as one of the first steps,” DeMaria says. “The initial challenge was erasing the clear dividing line between clinical engineering equipment and IT equipment. Just because it looks and feels like a PC, it is not always a PC. We now recognize that the skill sets and thought processes are different.”
After years of on-the-job learning, DeMaria applied to an online university 4 years ago to formally boost his own skill set and earn a degree in network security. He expects to finish the degree this year.
The entire staff at Olathe has been to basic vendor networking courses, and 95% of the clinical engineers are actively engaged in IT course work at the community college level. The by-product of better understanding is that the “us versus them” attitude is largely a thing of the past.
It is a good thing, because system-level integration, where devices are talking to other devices within the hospital network, has made cooperation more important than ever. “We are no longer seeing isolated LANS where radiology has its own little network,” DeMaria says. “We need to work closely with the IT folks, which means the role of the clinical engineer must continue to change. If a switch goes out, we are not just losing the e-mail network; we are losing patient monitoring.”
Even in a combined department, assigning “ownership” to a particular problem is crucial in the case of a “hand-off.” If IT works on a problem but later passes it on to clinical engineering, who is responsible for resolving the case?
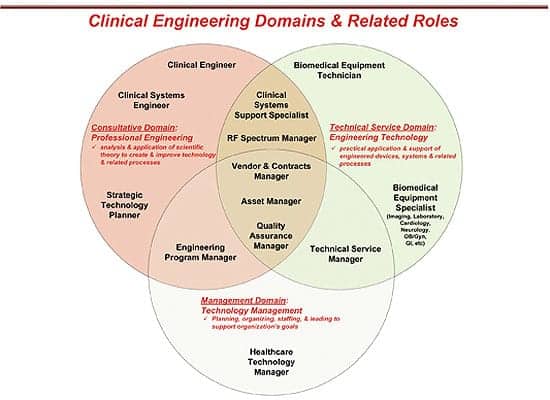
As convergence continues, there could be a spectrum of clinical engineering roles, possibly mirroring this sample chart (courtesy of S.L. Grimes).
“When clinical engineering finished their piece, they were reporting back to IT that the piece was done, but things got delayed because each side thought the other was moving forward with the issue,” DeMaria says. “The process of handing off ownership had to be worked out and documented so that both sides clearly knew when ownership was transferred to the other group. Acknowledgement of that handoff had to be made.”
Not so long ago, DeMaria says that clinical engineering used to worry solely about patient care, and cost considerations were secondary. Clinical engineering had a budget but did not always keep to it. “All that mattered was the patient,” DeMaria says. “The opposite of the spectrum can be found on the IT side, where things are very rule driven, process driven, and business driven—with not so much emphasis on patients or clinicians.”
Recognizing that IT does some things really well has sped up the evolution of the clinical engineer’s role. Change management is one example that has been cultivated within IT for years. For biomeds looking to alter the network and affect other devices, the IT commitment to communication has admittedly made everything smoother.
Meanwhile, the clinical engineering side is bringing a sense of urgency that IT administrators have lacked. “It’s OK to wait 5 minutes for e-mail,” DeMaria says. “It is not OK to wait 5 minutes for vital signs and patient monitoring.”
Part of that customer service mentality can be seen when clinicians call up clinical engineering at Olathe. Clinicians never hear the dreaded phrase, “That’s not my job.” Instead, clinical engineers take on the roles of facilitators and helpers—whether the problem is IT-related or not.
“I want my clinicians to be clinicians,” DeMaria stresses. “I don’t want them to have to determine whether they need to call the applications team or the network team or the IT team. Clinical engineering makes the determination as to whether we are experiencing a network issue, an application issue, or a clinical engineering issue. We route it to the right person, and we get it handled. That gives clinicians one phone number to call.”
Greg Thompson is a contributing writer for 24×7. For more information, contact .