Smart hospitals are controlling costs by rethinking notions of waste
Picture this: Alcoa, the global manufacturer of aluminum, sells sheet metal to Ball Corp. Ball Corp makes beverage cans for Coca-Cola. Coca-Cola stocks the grocery aisle at Walmart. Finally, Walmart sells the cola to you, and that’s where things start to get interesting: After you have refreshed yourself, you either toss the can into the trash or recycling.
Alcoa hopes you choose the latter, because recycling saves 90%1 of the energy needed to make aluminum from bauxite ore. That promise of efficiency is why a $13 billion2 market has developed around aluminum recycling, the complex logistics of transporting that empty Coke can from your kitchen back to an Alcoa blast furnace for reprocessing.
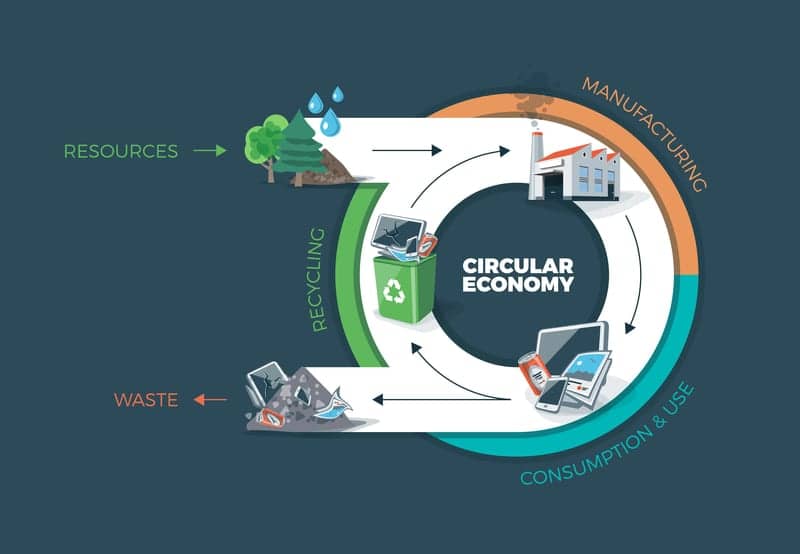
Business folks call it “closed-loop manufacturing,” and it’s part of what has become known as the circular economy.
The circular economy is an alternative to the linear “take, make, dispose” model that drives much of the world. Instead, raw materials, parts, and components are kept in the system as long as possible, providing higher value and utility over time. The Ellen MacArthur Foundation defines the circular economy philosophy through three core principles3:
- Preserving and enhancing natural capital by controlling limited supplies and balancing renewable resources
- Optimizing resource yields by ensuring that products, components, and materials continue contributing to the economy at all times
- Fostering system effectiveness by managing issues such as land use, air, water and noise pollution, release of toxic substances, and climate change
The imaging equipment business has no blast furnaces, and Coke cans pale in complexity compared to ultrasound or CT scanners. But we do have our own manifestation of the circular economy and its principles.
A typical hospital must track, maintain, and manage a fleet of imaging machines and parts with potentially millions of component combinations. It’s a multifaceted challenge keeping the hospital current with the latest available technology, knowing when systems may fail, determining when to repair and replace, selecting from new and repurposed parts, and staging herculean tasks (like deinstalling an MRI machine that weighs more than a London double-decker bus). Healthcare technology management long ago surpassed a mere “full-time job.” The market for refurbished medical equipment is projected to be worth $9.37 billion4 by 2019. It’s an industry.
It’s also a sea change from the ethos that guided previous generations of equipment manufacturing and management. Industrial designer Brooks Stevens famously coined the term “planned obsolescence,” the assumption that products would (and should) be replaced before the end of their useful lives. But the familiar “take, make, dispose” economic model relies on large quantities of cheap, easily accessible materials, and energy.
It could only have emerged in an era where Mad Men’s Don Draper bought a new Cadillac every year. Today, contemporary notions ranging from environmental stewardship to total cost of ownership have made clear that this consumption-based economic model is reaching its physical limits.
Cost, as always, is a key driver. A survey by the American College of Healthcare Executives (ACHE) reveals5 that seismic changes surrounding the healthcare industry have nudged “meeting the financials of running the business” to the top concern among hospital executives, ahead of considerations such as implementing healthcare reform and even patient safety and quality.
“Taking care of patients and improving patient safety and quality is job number one, but CEOs acknowledge they must do so in a climate of complex payment reform, dwindling reimbursement, and government mandates,” said Deborah J. Bowen, CEO of ACHE, in a statement that accompanied the 2015 release of the survey results.
In other words, it’s more important than ever for providers to navigate the delicate balance between delivering quality healthcare and controlling costs. Equipment maintenance and management—with an eye to optimizing resource yields—is an essential part of every healthcare industry executive’s solution.
To be sure, closing “the loop” in the medical equipment field remains an aspiration. According to GreenBiz,6 US hospitals generate more than two million tons of medical waste each year. The majority is lost, but medical equipment contains parts and components that can be repaired and reused. Once these parts have been stripped from the original equipment, we are left with a great deal of raw materials—copper, brass, aluminum, plastic, stainless steel—that can and should be recycled into the supply chain. Hazardous materials, such as mercury or lead, should never end up in landfills, but, of course, are often part of the unexamined waste stream.
Still, a circular economy approach offers tremendous gains for the healthcare provider, the equipment manufacturer and, ultimately, the patient. With a fully installed and properly functioning equipment management system, the provider increases the uptime, and therefore the revenue-generating availability, of crucial imaging equipment.
Adding reliable refurbished parts to the range of repair options reduces costs. And the circular economy approach can lengthen the interim between wholesale replacements of equipment while assuring the latest technology is in the hands of practitioners and at the service of patients.
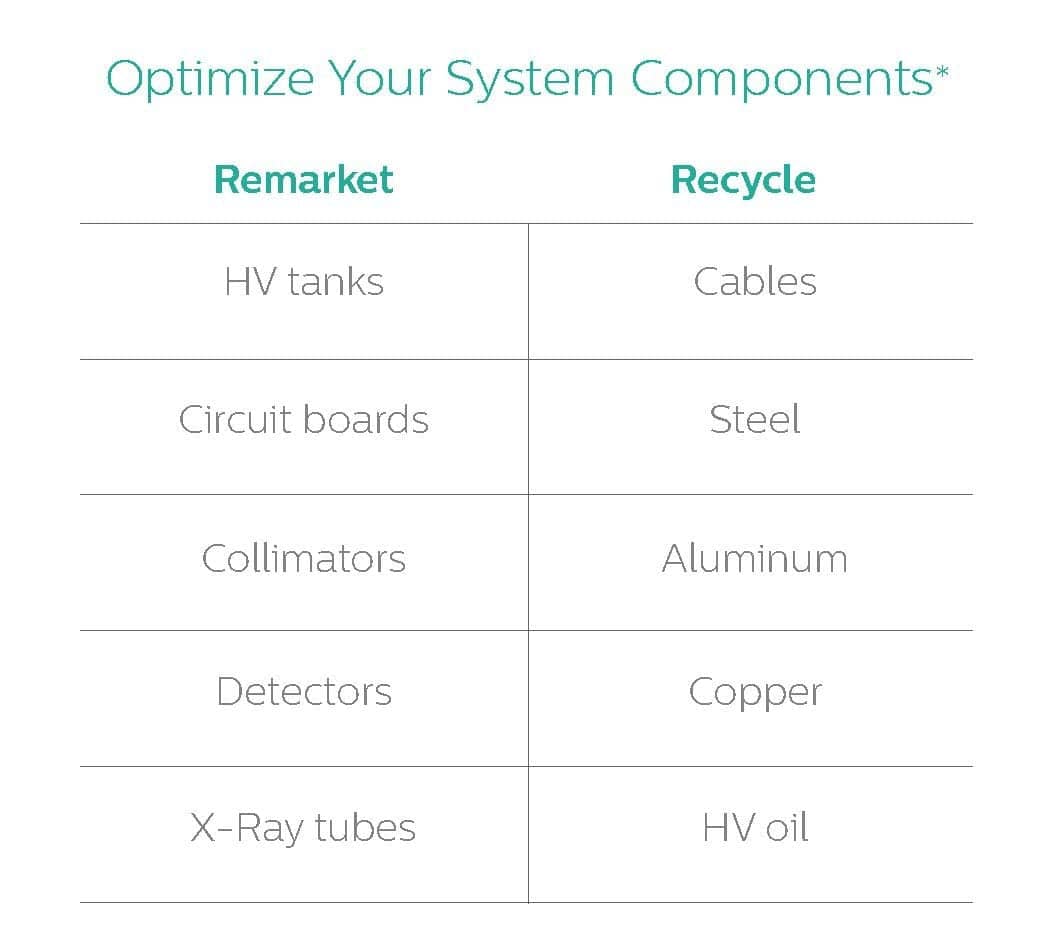
*An example based on typical end-of-life CT scan equipment and similar imaging products. (Click to enlarge)
At the end of the day, those tasked with managing and maintaining imaging systems or other medical equipment within the circular economy face two options: extension of equipment for additional utility or its disposal for parts and materials harvesting. Each path comes with its own set of questions, the answers to which require a sophisticated understanding of the field and the circular economy approach.
Extension. Should this CT system be repaired at all? Is the next generation of this technology an incremental or substantial advance? What components of this equipment will fail next? Are replacement parts available? Must we buy those new or are refurbished versions on the market? Is there a deep and accessible online catalogue of such parts? Is ordering available 24/7/365? Is tech support offered by my supplier?
Have available refurbished parts been adequately tested for reliability? What is the warranty rate of the refurbished parts supplier? What is the downtime to effect repairs? When are required parts available—next hour, day, or week? Do we have the expertise in-house to make determinations such as these? Should we seek outside counsel to train our internal staff? Would those partners service all, or just some, of our equipment?
Disposal. If the equipment is obsolete, redundant or beyond repair, how and when should the unit be decommissioned in a manner that causes the least disruption to the function of the provider facility?
Does the unit contain circuit boards, x-ray tubes, HV tanks, motors, transformers, cast aluminum, and components that may be useful in other equipment? Does the unit contain used oil, batteries, lead, mercury or materials that should be handled with environmental sensitivity?
Do we have the knowledge and tools (industrial copper wire strippers, for example) to extract from the equipment all the materials that may be repurposed and recycled? Will the disposal be conducted by technicians with ISO certification who will ensure compliance with pertinent regulations?
How long will the deinstallation take? What can be learned from the lifetime performance of this equipment, and what is revealed during deinstallation, that would inform the next generation of equipment design, function, or operation?
Healthcare organizations that view the management and maintenance of their equipment strategically recognize the value of viewing their assets through the lens of the circular economy. They understand the difference between “waste” and “perceived waste.” They realize that controlling costs and maintaining quality and reliability can be achieved in tandem and, ironically, by employing identical tactics. That’s why the industry of refurbished medical equipment is global, growing, and gaining ground.
Being guided by the precepts of the circular economy may seem daunting, but service partners who specialize in this field can ease the transition by leveraging their own knowledge, expertise, and infrastructure.
Is your service provider committed to bringing the circular economy to your equipment and maintenance program? If not, you may wish to find one that will.
Jim Salmons is vice president, Philips Multi-Vendor Services and AllParts Medical. For more information, contact chief editor Jenny Lower at [email protected].
References
1. Aluminum Recycling. (n.d.). Retrieved 2016, from http://www.aluminum.org/sustainability/aluminum-recycling
2. Pickard, J. (2014, May 1). Recycling Economics and Markets: Scrap Recycling Industry Trends and Outlook. Retrieved 2016, from http://www.cra-recycle.org/wp-content/uploads/2014/05/CRA-G1-Joe-Pickard.pdf
3. The principles of a circular economy. (2015). Retrieved 2016, from http://www.ellenmacarthurfoundation.org/circular-economy/overview/principles
4. Refurbished Medical Equipment Market worth $9.37 Billion by 2019. (2014). Retrieved 2016, from http://www.marketsandmarkets.com/PressReleases/refurbished-medical-devices.asp
5. Survey: Healthcare Finance, Reform Top Issues Confronting Hospitals in 2014. (2015, January 12). Retrieved 2016, from https://www.ache.org/pubs/Releases/2015/top-issues-confronting-hospitals-2014.cfm
6. Fleischer, D. (2015, August 6). 5 best practices to green healthcare. Retrieved 2016, from http://www.greenbiz.com/article/5-best-practices-green-healthcare
Photo credit: © Peter Varga | Dreamstime.com